




Labor consists of a series of rhythmic, involuntary or medically induced contractions of the uterus that result in effacement (thinning and shortening) and dilation of the uterine cervix. In 1996, the World Health Organization (WHO) defined normal birth as follows (1):
The birth is spontaneous in onset and low risk at the start of labor and remains so throughout labor and delivery.
The infant is born spontaneously in the vertex position between 37 and 42 weeks of pregnancy.
After birth, mother and infant are in good condition.
The stimulus for labor is unknown, but digitally manipulating or stretching the cervix during examination enhances uterine contractile activity, most likely by stimulating release of oxytocin by the posterior pituitary gland.
In uncomplicated term pregnancies, labor usually begins within 2 weeks (before or after) of the estimated date of delivery. In a first pregnancy, labor lasts 12 to 18 hours on average; subsequent labors are often shorter, averaging 6 to 8 hours.
Management of labor protraction or arrest requires additional measures (eg, induction or augmentation of labor, forceps or vacuum extractor delivery, cesarean delivery).
(See also Introduction to Intrapartum Complications.)
General reference
1. Care in normal birth: A practical guide. Technical Working Group, World Health Organization. Birth 24(2):121-123, 1997.
Birthing Options
Settings for childbirth vary. Patients may have options of delivering at a hospital, birthing center, or at home. Hospital delivery has the advantage of having clinical staff and equipment immediately available if unexpected maternal and fetal complications occur during labor and delivery (eg, placental abruption, shoulder dystocia, need for emergency cesarean delivery, fetal or neonatal distress or abnormality) or postpartum (eg, postpartum hemorrhage).
For many women, presence of their partner or another support person (eg, doula or perinatal support specialist) during labor is helpful and should be encouraged. Moral support and encouragement may decrease anxiety. Childbirth education classes can prepare parents for labor and delivery, including providing information about normal labor, monitoring equipment, and potential complications.
Beginning of Labor
Labor usually begins with irregular uterine contractions of varying intensity and the cervix begins to efface and dilate. As labor progresses, contractions increase in duration, intensity, and frequency. Sometimes the chorioamniotic membranes rupture before the onset of contractions.
Bloody show (a small amount of blood with mucous discharge from the cervix) may be an early sign the labor will soon begin. However, bloody show may also occur as a result of sexual intercourse. Bloody show may precede onset of labor by as much as 72 hours. Any vaginal bleeding in pregnancy should be assessed to exclude complications. With bloody show, the amount of blood is very small and mucus is typically present, which usually differentiates it from abnormal third-trimester vaginal bleeding.
Typically, pregnant women are advised to call their health care team or go to the hospital if they believe their membranes have ruptured or if they are experiencing contractions lasting at least 30 seconds and occurring regularly at intervals of about 6 minutes or less for an hour. Patients are evaluated, and if it is uncertain whether labor has begun, they are observed for a time and sent home if labor has not begun.
Symptoms that are not associated with normal labor, such as persistent (rather than intermittent) abdominal or back pain, heavy vaginal bleeding, or hemodynamic instability, that suggest placental abruption (premature separation of the placenta) require immediate evaluation and management. Placenta previa is typically ruled out with routine prenatal ultrasonography in the second trimester. However, if the location of the placenta is unknown or the placenta was low-lying on the most recent ultrasound, digital vaginal examination is contraindicated, and ultrasonography should be done as soon as possible.
Admission to Labor Unit
When a pregnant patient is admitted to the labor unit, vital signs are measured. Blood is drawn for a complete blood count (CBC), blood typing, and antibody screening. If routine laboratory tests were not done during prenatal visits, they should be done. These tests include screening for HIV, hepatitis B, and syphilis; testing rubella and varicella immunity; and group B streptococcal infection.
The presence and rate of fetal heart sounds are recorded. A physical examination is done. While examining the abdomen, the clinician estimates size, position, and presentation of the fetus, using the Leopold maneuver (see figure Leopold Maneuver). If fetal presentation or lie is uncertain, ultrasonography may be done.
If labor is active, patients should receive little or nothing by mouth to prevent possible vomiting and aspiration during delivery or in case emergency delivery with general anesthesia is necessary. Some health facilities permit clear liquids in low-risk patients.
Shaving or clipping of vulvar and pubic hair is not indicated, and it increases the risk of wound infections.
An IV infusion of Ringer's lactate may be started, preferably using a large-bore indwelling catheter inserted into a vein in the hand or forearm. During a normal labor of 6 to 10 hours, women should be given 500 to 1000 mL of this solution. The infusion prevents dehydration during labor and subsequent hemoconcentration and maintains an adequate circulating blood volume. The catheter also provides immediate access for medications or blood products if needed. Fluid preloading is valuable if epidural or spinal anesthesia is planned.
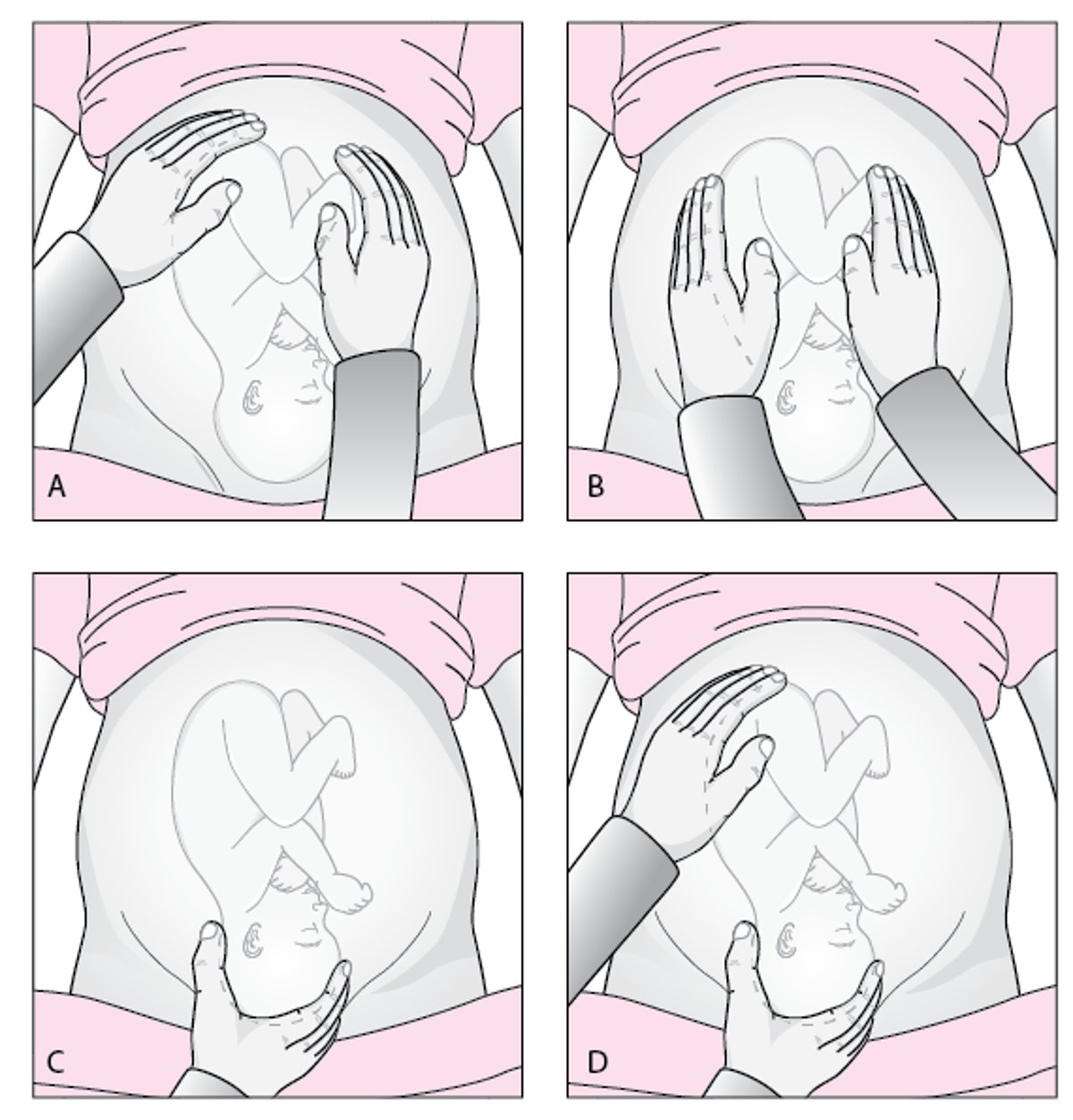
Leopold Maneuver
(A) The uterine fundus is palpated to determine which fetal part occupies the fundus. (B) Each side of the maternal abdomen is palpated to determine which side is fetal spine and which is the extremities. (C) The area above the symphysis pubis is palpated to locate the fetal presenting part and thus determine how far the fetus has descended and whether the fetus is engaged. (D) One hand applies pressure on the fundus while the index finger and thumb of the other hand palpate the presenting part to confirm presentation and engagement. |

If there are concerns about complications after the initial examination, fetal monitoring, and laboratory tests, additional testing or monitoring is done.
If the pregnancy is preterm (< 37 weeks) and patients present with uterine contractions or leaking of fluid, they are assessed for preterm labor or preterm prelabor rupture of membranes and managed accordingly.
Cervical Examination
If the patient has regular, painful contractions, a cervical examination is done to assess cervical dilation.
In patients with placenta previa, cervical examination can cause severe hemorrhage and, therefore, is not done. If placental location has not been determined during prenatal care, ultrasonography should be done before a pelvic examination.
Cervical dilation is recorded in centimeters as the diameter of a circle; 10 cm is considered fully dilated.
Effacement is estimated in percentages, from zero to 100%. Because effacement involves cervical shortening as well as thinning, it may be recorded in centimeters using the normal, uneffaced average cervical length of 3.5 to 4.0 cm as a guide.
Station is expressed in centimeters above or below the level of the maternal ischial spines. Level with the ischial spines corresponds to 0 station. Levels below the ischial spines are documented as (+); levels higher in the pelvis above the ischial spines are documented as (−). Levels are recorded in centimeter increments.
Fetal lie, position, and presentation are noted.
Lie describes the relationship of the long axis of the fetus to that of the mother (longitudinal, oblique, transverse).
Position describes the relationship of the presenting part to the maternal pelvis (eg, occiput left anterior for cephalic, sacrum right posterior for breech).
Presentation describes the part of the fetus at the cervical opening (eg, breech, vertex, shoulder).
Abnormal fetal lie, position, or presentation may be associated with intrapartum complications.
Rupture of Membranes
Occasionally, the membranes (amniotic and chorionic sac) rupture before labor begins, and amniotic fluid leaks through the cervix. Rupture of membranes at any stage before the onset of labor is called prelabor rupture of membranes (PROM). Some women with PROM feel a gush of fluid from the vagina, followed by steady leaking (1).
If the patient presents with possible rupture of membranes, but does not have regular and painful contractions, a sterile speculum examination is done initially to confirm rupture of membranes. To decrease the risk of infection, digital cervical examinations are delayed until it appears that labor has begun or if there are other indications to assess cervical dilation (eg, planning labor induction).
Further confirmation is sometimes needed to differentiate amniotic fluid from other fluids (eg, urine, vaginal discharge, semen). Rupture of membranes can be confirmed on pelvic examination if fluid is seen leaking from the cervix, and there is pooling in the posterior vagina. Fetal meconium (producing greenish-brown discoloration) should be noted if present, because it may be a sign of fetal stress.
If pooling is not seen, confirmation may require testing. For example, the pH of vaginal fluid may be tested with nitrazine paper, which turns deep blue at a pH >2, 3).
If rupture is still unconfirmed, ultrasonography showing oligohydramnios (deficient amniotic fluid) provides further evidence suggesting rupture. Rarely, amniocentesis with instillation of dye is done to confirm rupture; dye detected in the vagina or on a tampon confirms rupture.
About 80 to 90% of women with PROM at term ( ≥ 37 weeks) and about 50% of women with preterm PROM (< 37 weeks) go into labor spontaneously within 24 hours; > 90% of women with PROM go into labor within 2 weeks. If membranes rupture at term but labor does not start within several hours, labor is typically induced to lower risk of maternal and fetal infection. When preterm PROM occurs (at < 37 weeks), the delay between rupture and labor onset increases with decreasing gestational age.
Rupture of membranes references
1. Prelabor Rupture of Membranes: ACOG Practice Bulletin, Number 217. Obstet Gynecol 135(3):e80-e97, 2020. doi:10.1097/AOG.0000000000003700
2. Ramsauer B, Vidaeff AC, Hösli I, et al: The diagnosis of rupture of fetal membranes (ROM): a meta-analysis. J Perinat Med. 2013;41(3):233-240. doi:10.1515/jpm-2012-0247
3. Thomasino T, Levi C, Draper M, Neubert AG. Diagnosing rupture of membranes using combination monoclonal/polyclonal immunologic protein detection. J Reprod Med. 2013;58(5-6):187-194.
Stages of Labor
There are 3 stages of labor.
First stage
The first stage—from onset of labor to full dilation of the cervix (about 10 cm)—has 2 phases, latent and active.
The latent phase is the interval from the onset of labor to the onset of the active phase (1). Irregular contractions become regular and more intense, discomfort is mild to moderate, and the cervix effaces and begins to dilate to 4 to 6 cm. The latent phase is difficult to define precisely and duration varies. For nulliparas, the mean is 7.3 to 8.6 hours (95th percentile, 17 to 21 hours) (2). For multiparas, the mean is 4.1 to 5.3 hours (95th percentile, 12 to 14 hours).
There is no standard definition of a protracted latent phase. A commonly used standard is > 20 hours in nulliparous patients or > 14 hours in multiparous patients, although some studies have reported shorter and longer durations (3).
The active phase is defined by accelerated cervical dilation. Regular contractions continue until the cervix becomes fully dilated.
Active-phase protraction is diagnosed when, after 6 cm dilation is reached, the cervix dilates < 1.2 cm/hour in nulliparous patients or < 1.5 cm/hour in multiparous patients (4). Active-phase arrest is typically defined as no change in cervical dilation for 2 to 4 hours.
Pelvic examinations are done as needed in the latent phase and typically every 2 to 3 hours in the active phase to evaluate labor progress.
Standing and walking shorten the first stage of labor by > 1 hour and reduce the rate of cesarean delivery (5).
If the membranes have not spontaneously ruptured, some clinicians use amniotomy (artificial rupture of membranes) routinely during the active phase. As a result, labor may progress more rapidly, and meconium-stained amniotic fluid may be detected earlier. Amniotomy during this stage may be necessary for specific indications, such as facilitating internal fetal monitoring to confirm fetal status. Amniotomy should be avoided in women with HIV infection or hepatitis B or C, so that the fetus is not exposed to these infections.
During the first stage of labor, maternal heart rate and blood pressure should be monitored frequently, and fetal heart rate should be checked continuously by electronic monitoring or intermittently by auscultation, usually with a portable Doppler ultrasound device (see fetal monitoring). Women may begin to feel the urge to bear down as the presenting part descends into the pelvis. However, they should be discouraged from bearing down until the cervix is fully dilated so that they do not tear or cause swelling of the cervix.
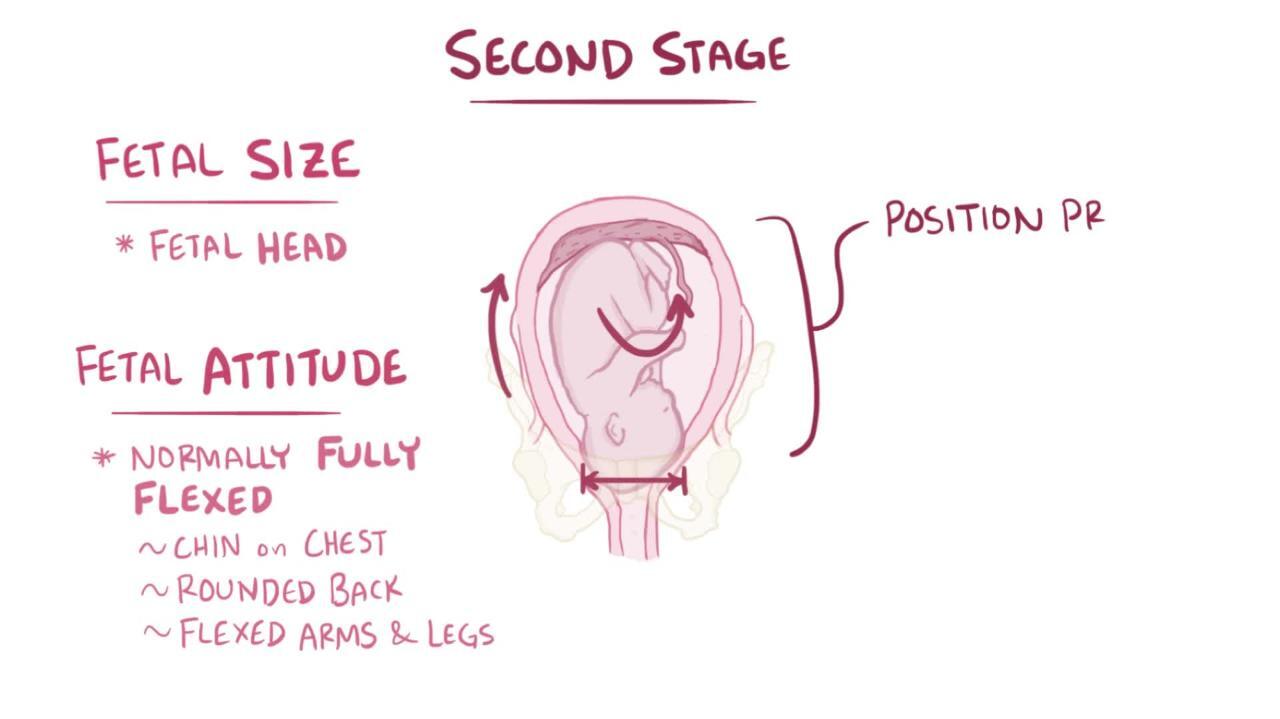
Second stage
The second stage of labor is the time from full cervical dilation to delivery of the fetus. Mean duration is 36 to 57 minutes in nulliparous patients (95th percentile, 122 to 197 minutes) and 17 to 19 minutes in multiparous patients (95th percentile, 57 to 81 minutes) (2). For spontaneous delivery, women must supplement uterine contractions by expulsively bearing down. In the second stage, women should be attended constantly, and fetal heart sounds should be checked continuously or after every contraction. Contractions may be monitored by palpation or electronically.
During the second stage of labor, perineal massage with lubricants and warm compresses may soften and stretch the perineum and thus reduce the rate of third- and fourth-degree perineal tears (6). These techniques are widely used by midwives and birth attendants.
During the second stage, the mother's position does not affect duration or mode of delivery or maternal or neonatal outcome in deliveries without epidural anesthesia (7). Also, the pushing technique (spontaneous versus directed and delayed versus immediate) does not affect the mode of delivery or maternal or neonatal outcome.
Second-stage arrest is typically defined as at least 3 hours of pushing in nulliparous women or at least 2 hours in multiparous women (8). Use of epidural anesthesia delays pushing and may lengthen the second stage by an hour (9). Duration of pushing may also be longer due to malposition (eg, occiput posterior).

Third stage
The third stage of labor begins after delivery of the infant and ends with delivery of the placenta. This stage usually lasts only a few minutes but may last up to 30 minutes.
Stages of labor references
1. American College of Obstetricians and Gynecologists (ACOG): Obstetrics Data Definitions
2. Kilpatrick SJ, Garrison E, Fairbrother E: Normal labor and delivery. In: Landon MB, Galan HL, Jauniaux E, et al, eds. Gabbe's Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021. eBook ISBN: 9780323613408
3. Tilden EL, Phillippi JC, Ahlberg M, et al: Describing latent phase duration and associated characteristics among 1281 low-risk women in spontaneous labor. Birth 46(4):592-601, 2019. doi:10.1111/birt.12428
4. Friedman EA, Cohen WR. The active phase of labor. Am J Obstet Gynecol. 2023;228(5S):S1037-S1049. doi:10.1016/j.ajog.2021.12.269
5. Lawrence A, Lewis L, Hofmeyr GJ, Styles C: Maternal positions and mobility during first stage labour. Cochrane Database Syst Rev (8):CD003934, 2013. doi: 10.1002/14651858.CD003934.pub3
6. Aasheim V, et al: Perineal techniques during the second stage of labour for reducing perineal trauma. Cochrane Database Syst Rev 6:CD006672, 2017. doi: 10.1002/14651858.CD006672.pub3
7. Gupta JK, Sood A, Hofmeyr GJ, et al: Position in the second stage of labour for women without epidural anaesthesia. Cochrane Database Syst Rev 5:CD002006, 2017. doi: 10.1002/14651858.CD002006.pub4
8. Obstetric care consensus no. 1: safe prevention of the primary cesarean delivery. Obstet Gynecol. 123(3):693-711, 2014. doi:10.1097/01.AOG.0000444441.04111.1d
9. Lemos A, Amorim MM, Dornelas de Andrade A, et al: Pushing/bearing down methods for the second stage of labour. Cochrane Database Syst Rev 3:CD009124, 2017. doi: 10.1002/14651858.CD009124.pub3






