




Dizziness is an inexact term people often use to describe various related sensations, including
Faintness (feeling about to pass out)
Light-headedness
Dysequilibrium (feeling off balance or unsteady)
A vague spaced-out or swimmy-headed feeling
Vertigo (a sensation of movement when there is no actual movement)
Vertigo is a type of dizziness felt as a sensation of movement when there is no actual movement. People usually feel that they, their environment, or both are spinning. The feeling is similar to that produced by the childhood game of spinning round and round, then suddenly stopping and feeling the surroundings spin. Occasionally, people simply feel pulled to one side. Vertigo is not a diagnosis. It is a description of a sensation.
People with vertigo may also have nausea and vomiting, difficulty with balance, and/or trouble walking. Some people have a rhythmic jerking movement of the eyes (nystagmus) during an episode of vertigo.
Different people often use the terms “dizziness” and “vertigo” differently, perhaps because these sensations are hard to describe in words. Also, people may describe their sensations differently at different times. For example, the sensations might feel like light-headedness one time and like vertigo the next.
However it is described, these sensations can be disturbing and even incapacitating, particularly when accompanied by nausea and vomiting. Symptoms cause particular problems for people doing an exacting or dangerous task, such as driving, flying, or operating heavy machinery.
Dizziness accounts for about 5 to 6% of doctor visits. It may occur at any age but becomes more common as people age. It affects about 40% of people older than 40 at some time. Dizziness may be temporary or chronic. Dizziness is considered chronic if it lasts more than a month. Chronic dizziness is more common among older people.
For dizziness that occurs only on standing up, see Dizziness or Light-Headedness When Standing Up.
Did You Know...
|
Causes of Dizziness and Vertigo
Vertigo is usually caused by disorders of the parts of the ear and brain that are involved in maintaining balance:
Brain stem and cerebellum
Nerve tracts connecting the inner ear to the brain stem and cerebellum
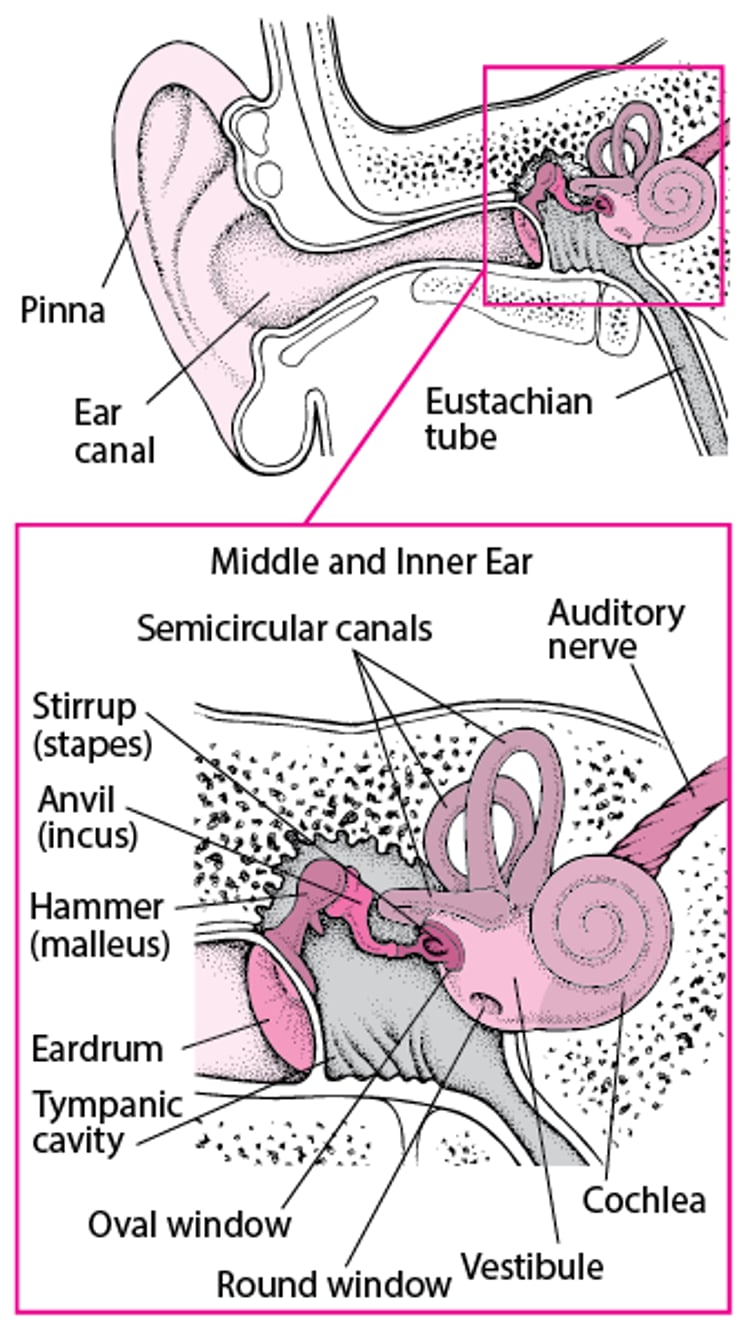
The inner ear contains structures (the semicircular canals, saccule, and utricle) that enable the body to sense position and motion. Information from these structures is sent to the brain through the vestibulocochlear nerve (8th cranial nerve, which is also involved in hearing). This information is processed in the brain stem, which adjusts posture, and the cerebellum, which coordinates movements, to provide a sense of balance. A disorder in any of these structures can cause vertigo. Disorders of the inner ear sometimes also cause decreased hearing and/or ringing in the ear (tinnitus). (See figure A Look Inside the Ear.)
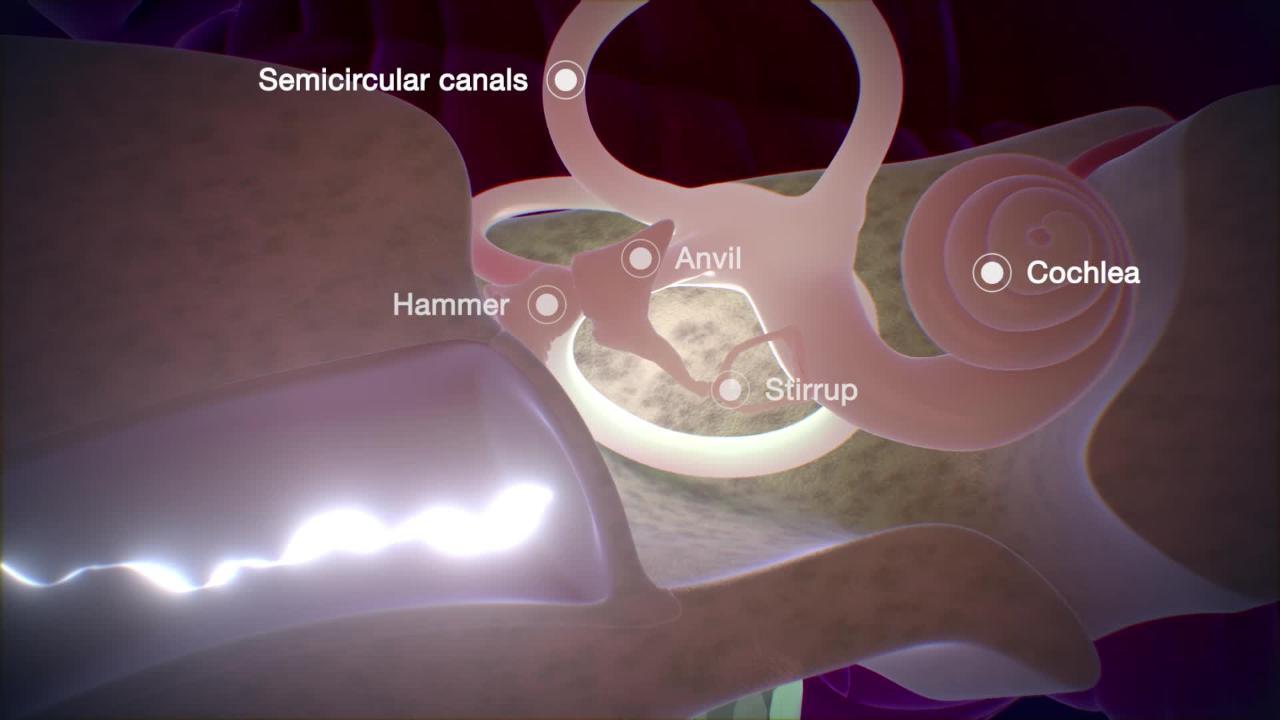
A Look Inside the Ear

Also, any disorder that affects brain function in general (for example, low blood sugar, low blood pressure, severe anemia, or many drugs) can make people feel dizzy. Although symptoms may be disturbing and even incapacitating, only a small percentage of cases result from a serious disorder.
Common causes
Although there is some overlap, causes of dizziness can roughly be divided into those with and without vertigo.
The most common causes of dizziness with vertigo include the following:
Vestibular migraine headache
Vestibular migraine headache is increasingly recognized as a common cause of dizziness with vertigo. This type of migraine most often occurs in people who have a history or family history of migraines. People often have headache with the vertigo or dizziness. Some have other migraine-like symptoms, such as seeing flashing lights, having temporary blind spots, or being very sensitive to light and sound. People may also have hearing loss, but it is not a common symptom.
The most common causes of dizziness without vertigo include the following:
Drug effects
Multifactorial causes
Several kinds of drugs can cause dizziness. Some drugs are directly toxic to the nerves of the ears and/or balance organs (ototoxic drugs). These drugs tend to cause dizziness and an inability to focus on a visual target (oscillopsia). Other drugs, for example, sedatives, affect the brain as a whole. In older people, dizziness often is due to several factors, usually a combination of drug side effects plus an age-related decrease in sensory function.
Dizziness without vertigo may occur when the brain receives insufficient oxygen and glucose (low blood sugar), such as may be related to nonneurologic disorders including heart and lung disorders or severe anemia.
People with panic disorder, shortness of breath, anxiety, or depression may experience dizziness.
Very often, no particular cause is found, and symptoms go away without treatment.
Less common causes
Less common causes of dizziness include a tumor of the vestibulocochlear nerve (vestibular schwannoma); a tumor, stroke, or transient ischemic attack (TIA) affecting the brain stem; an injury to the eardrum, inner ear, or base of the skull; multiple sclerosis; and pregnancy.
Evaluation of Dizziness and Vertigo
The following information can help people with dizziness decide whether a doctor’s evaluation is needed and help them know what to expect during the evaluation.
Warning signs
In people with dizziness, certain symptoms and characteristics are cause for concern. They include
Headache
Neck pain
Difficulty walking
Loss of consciousness (fainting)
Other neurologic symptoms (such as trouble hearing, seeing, speaking, or swallowing or difficulty moving an arm or leg)
When to see a doctor
People who have warning signs, those whose symptoms are severe or have been continuous for over an hour, and those with vomiting should go to a hospital right away. Other people should see their doctor as soon as possible. People who had a single, brief (less than 1 minute), mild episode with no other symptoms may choose to wait and see whether they have another episode.
What the doctor does
In people with dizziness, doctors first ask questions about the person's symptoms and medical history. Doctors then do a physical examination. What they find during the history and physical examination often suggests a cause of the dizziness and the tests that may need to be done (see table Some Causes and Features of Dizziness).
In addition to warning signs, important features that doctors ask about include severity of the symptoms (has the person fallen or missed work), presence of vomiting and/or ringing in the ears, whether symptoms come and go or have been continuous, and possible triggers of the symptoms (for example, changing position of the head or taking a new drug).
During the physical examination, the ear, eye, and neurologic examinations are particularly important. Hearing is tested, and the ears are examined for abnormalities of the ear canal and eardrum. The eyes are checked for abnormal movements, such as nystagmus.
Hearing loss or ringing in the ears (tinnitus) suggests that people may have a disorder of the inner ear.
Nystagmus suggests a disorder affecting the inner ear or various nerve connections in the brain stem. With nystagmus, the eyes rapidly and repeatedly jerk in one direction and then return more slowly to their original position. Doctors deliberately try to trigger nystagmus if people do not have it spontaneously because the direction in which the eyes move and how long the nystagmus lasts help doctors diagnose the cause of vertigo. To trigger nystagmus, doctors first lay people on their back and gently roll them from side to side while watching their eyes. Specialists sometimes have the person wear thick, one-way, magnifying glasses called Frenzel lenses. Doctors can easily see the person's magnified eyes through the lenses, but the person sees a blur and cannot visually fixate on anything (visual fixation makes it harder to trigger nystagmus). During the maneuver to induce nystagmus, eye movements may be recorded by using electrodes (sensors that stick to the skin) placed around each eye (electronystagmography) or by a video camera attached to the Frenzel lenses (video electronystagmography). If no nystagmus occurs with rolling side to side, doctors try other maneuvers. These other maneuvers include putting ice-cold water into the ear canal (caloric testing) and rapidly changing the position of the person's head (Dix-Hallpike maneuver).
Doctors also do a complete neurologic examination, paying particular attention to tests of walking, balance, and coordination.
Testing
The need for tests in people with dizziness or vertigo depends on what doctors find during the history and physical examination, particularly whether warning signs are present.
For people with a sudden attack of dizziness that is still going on, doctors usually apply a fingertip oxygen sensor, measure blood glucose from a drop of blood from the fingertip. Some women get a pregnancy test.
People with warning signs typically require gadolinium-enhanced magnetic resonance imaging (MRI), as do people without warning signs who have had symptoms for a long time.
Several tests can be used to evaluate balance and gait, such as the Romberg test. Another test of balance has the person walking a straight line with one foot behind the other. If the doctor's examination shows possible hearing loss, people are usually sent for a formal hearing test (audiogram).
Comprehensive vestibular testing is sometimes done. This testing includes video electronystagmography (computerized recording and analysis of abnormal eye movements), rotary chair testing (looking for abnormal eye movements while sitting in a chair that is rotated), and vestibular-evoked myogenic potential testing. These tests are typically done by doctors who specialize in the care of the ear (otolaryngologists).
Electrocardiography (ECG), Holter monitoring for heart rhythm abnormalities, echocardiography, and exercise stress testing may be done to evaluate heart function. For dizziness that occurs only when standing up, specific tests may be needed.
Treatment of Dizziness and Vertigo
The cause of dizziness is treated whenever possible. Treatment includes stopping or reducing the dose of any drug that is the cause or switching to an alternative drug.
Vertigo caused by disorders of the inner ear, such as Meniere disease, labyrinthitis, migraine associated vertigo, or vestibular neuronitis
Vertigo in people with benign paroxysmal positional vertigo is treated with the Epley maneuver (a somersault-like maneuver of the head) done by an experienced practitioner. Sometimes, people learn how to do this at home to help relieve symptoms if they recur.
Meniere disease is best managed by an otolaryngologist with training in management of this chronic disorder, but initial management consists of a low-salt diet and a diuretic ("water pills"), which may not be effective in all people with the disorder.
In people with vertigo that occurs with migraines, the migraine is treated.
If vertigo persists for a long time, some people benefit from physical therapy to help them cope with their disturbed sense of balance. Therapists may also recommend such strategies as
Avoiding movements that may trigger dizziness, such as looking up or bending down
Storing items at levels that are easy to reach
Getting up slowly after sitting or lying down
Clenching hands and flexing feet before standing
Learning exercises that combine eye, head, and body movements to help prevent dizziness
Doing physical therapy and exercises to strengthen muscles and maintain independent gait as long as possible
Undergoing vestibular rehabilitation therapy (a specialized form of physical therapy that targets symptoms of peripheral and central vestibular dysfunction)
Essentials for Older People
As people grow older, many factors make dizziness and vertigo more common. The organs involved in balance, particularly the structures of the inner ear, function less well. It becomes harder to see in dim light. The body's mechanisms that control blood pressure respond more slowly (for example, to standing up). Older people are also more likely to be taking drugs that can cause dizziness.
Although dizziness and vertigo are unpleasant at any age, they cause particular problems for older people. Frail people have a much higher risk of falling and of sustaining serious injuries when they are dizzy. Even if they do not fall, their fear of falling often significantly affects their ability to do daily activities.
The drugs that help relieve vertigo can make people feel sleepy. This effect is more common and sometimes more severe in older people.
Even more so than younger people, older people with dizziness or vertigo may benefit from general physical therapy and exercises to strengthen their muscles to help them maintain their independence. Physical therapists can also provide important safety information for older or disabled people to help prevent falls.
Key Points
Dizziness and vertigo often result from disorders that affect the inner ear or the parts of the brain involved in balance or from use of certain prescription drugs.
Symptoms may include faintness, loss of balance, vertigo, difficult-to-describe light-headed or swimming sensations, or a combination.
Severe headache and any sign of difficulty with brain function (such as difficulty walking, talking, seeing, speaking, or swallowing) are warning signs, but even vague symptoms may result from a serious disorder.
People with warning signs should see a doctor right away, and they often require testing.






