




Subacute meningitis is inflammation of the layers of tissue that cover the brain and spinal cord (meninges) and of the fluid-filled space between the meninges (subarachnoid space) when it develops over days to a few weeks. Chronic meningitis is slowly developing meningitis that lasts 4 weeks or longer.
Many infections and disorders that cause inflammation can cause chronic meningitis.
Having a weakened immune system increases the risk of developing chronic meningitis.
Symptoms are usually similar to those of acute bacterial meningitis (headache, fever, and stiff neck) but may also include confusion, hearing loss, and double vision.
To diagnose chronic meningitis, doctors usually do imaging of the head, such as CT or magnetic resonance imaging (MRI), followed by a spinal tap (lumbar puncture) with analysis of the cerebrospinal fluid.
The cause is treated.
(See also Introduction to Meningitis.)
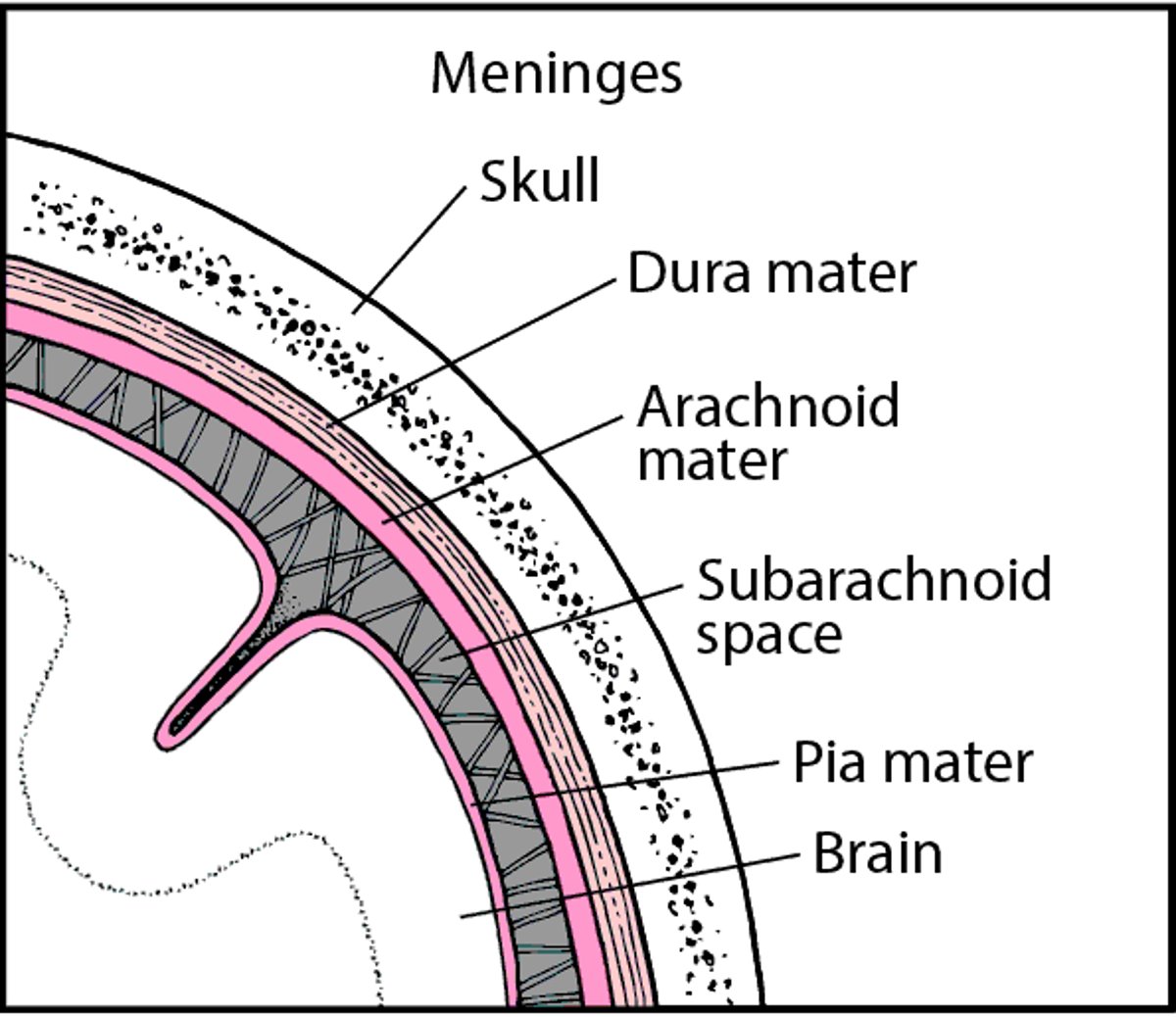
The brain and spinal cord are covered by three layers of tissue called meninges. The subarachnoid space is located between the middle layer and the inner layer of the meninges, which cover the brain and spinal cord. This space contains the cerebrospinal fluid, which flows through the meninges, fills the spaces within the brain, and helps cushion the brain and spinal cord.
Tissues Covering the Brain
Within the skull, the brain is covered by three layers of tissue called the meninges. |

Subacute meningitis develops over a longer period of time than acute meningitis and over a shorter period than chronic—over days to a few weeks. Its causes, symptoms, diagnosis, and treatment are similar to those of chronic meningitis. Bacterial meningitis may be subacute rather than acute.
Chronic meningitis develops slowly, over weeks or longer, and may last for months to years. Rarely, chronic meningitis causes only mild symptoms and resolves on its own.
Causes of Subacute and Chronic Meningitis
Subacute or chronic meningitis is usually caused by an infection. Many microorganisms can cause subacute or chronic meningitis. Among the most important microorganisms are
Bacteria that cause tuberculosis (Mycobacterium tuberculosis)
Bacteria that cause Lyme disease (Borrelia burgdorferi)
Fungi, including Cryptococcus neoformans, Cryptococcus gattii, Coccidioides immitis, Histoplasma capsulatum, and Blastomyces
Up to 8% of children and some adults with Lyme disease develop meningitis. Meningitis due to Lyme disease may be acute or chronic. Usually, it begins more slowly than acute viral meningitis.
The most common cause of chronic meningitis in the Western hemisphere is
Cryptococcus neoformans (which causes cryptococcosis)
These fungi are more likely to cause meningitis in people who have a weakened immune system due to disorders such as human immunodeficiency virus (HIV) infection or AIDS or who take drugs that suppress the immune system. Symptoms of meningitis due to Cryptococcus neoformans begin gradually and subtly, and they may come and go.
Less commonly, chronic meningitis is caused by the following:
Other bacteria (such as those that cause syphilis)
Fungi such as Coccidioides immitis (which causes coccidioidomycosis)
Parasites such as the protozoa Toxoplasmosis gondii (which causes toxoplasmosis), usually in people with HIV infection or AIDS
Viruses, such as HIV and enteroviruses
Chronic meningitis is common among people who have HIV infection. Meningitis can result from the HIV infection. But many other organisms (including Cryptococcus neoformans, Mycobacterium tuberculosis, and several fungi) can also cause chronic meningitis in people with HIV infection.
Disorders that are not infections can also cause chronic meningitis. They include
Certain disorders that cause inflammation, such as systemic lupus erythematosus (lupus), rheumatoid arthritis, Behçet syndrome, and Sjögren syndrome
Leukemia, lymphoma, breast cancer, lung cancer, melanoma, or other cancers that spread to the meninges
Occasionally, chronic meningitis persists for months or even years, but no organisms are identified, and death does not result. This type of meningitis is called chronic idiopathic meningitis. Treatment with antifungal drugs or corticosteroids does not help. However, some people with chronic idiopathic meningitis eventually recover without treatment.
Symptoms of Subacute and Chronic Meningitis
The symptoms of subacute or chronic meningitis are similar to those of acute bacterial meningitis, except that they develop more slowly and gradually, usually over weeks rather than days. Also, fever is often less severe. Symptoms of chronic meningitis may last for years. Some people get better for a while, then worsen (relapse).
Headache, confusion, a stiff neck, and back pain are common. People may have difficulty walking. Weakness, pins-and-needles sensations, numbness, paralysis of the face, and double vision are also common. Paralysis of the face, double vision, and hearing loss develop when meningitis affects the cranial nerves (which go directly from the brain to various parts of the head, neck, and trunk).
Meningitis due to the bacteria that cause tuberculosis usually worsens fairly rapidly (over days to weeks) but may develop much more rapidly or gradually. Tuberculous meningitis can have serious effects. Pressure within the skull may increase. Blood vessels may become inflamed, sometimes leading to stroke. Vision, hearing, facial muscles, and balance may be affected.
Diagnosis of Subacute and Chronic Meningitis
Spinal tap and analysis of cerebrospinal fluid
Doctors ask about factors that increase the risk of chronic meningitis, such as a weakened immune system (as may be caused by HIV infection or AIDS) and travel to areas where Lyme disease or certain fungal infections are common. Doctors also ask about and look for symptoms that may suggest a cause.
To confirm the diagnosis, doctors do a spinal tap (lumbar puncture) to obtain a sample of cerebrospinal fluid, which is then analyzed.
Analysis of cerebrospinal fluid
The cerebrospinal fluid is sent to a laboratory to be examined and analyzed. In people with meningitis, the number of white blood cells in cerebrospinal fluid is higher than normal. The results can usually enable doctors to distinguish between chronic and acute meningitis. Some infectious organisms that cause chronic meningitis, such as the fungus Cryptococcus neoformans, are visible under a microscope, but many, such as the bacteria that cause tuberculosis, are difficult to detect.
The cerebrospinal fluid is also cultured. Organisms, if present, are grown so that they can be identified. However, culturing may take weeks. Special techniques, which may provide results more quickly, may be used to identify fungi and the bacteria that cause tuberculosis and syphilis. For example, tests may be done to detect proteins released by Cryptococcus neoformans (called antigen testing).
The polymerase chain reaction (PCR) technique, which produces many copies of a gene, may identify the unique DNA sequence of the bacteria that cause tuberculosis. Doctors may also use an automated test called Xpert MTB/RIF, recommended by the World Health Organization (WHO) for the diagnosis of tuberculous meningitis, to detect the genetic material (DNA) of tuberculosis bacteria in samples of cerebrospinal fluid. Other tests may be done on samples of cerebrospinal fluid to document prior exposure to the bacteria that cause tuberculosis. Chest x-rays or computed tomography (CT) of the chest may detect evidence of prior or current tuberculosis.
Other tests on cerebrospinal fluid are done, depending on which disorders are suspected. For example, the fluid may be analyzed for cancer cells if cancer is suspected.
The cause of chronic meningitis may be difficult to determine, partly because detecting microorganisms in cerebrospinal fluid can be difficult. Thus, spinal taps may be repeated to obtain more cerebrospinal fluid for culture. If available, tests that can rapidly analyze large stretches of genetic material can be used to identify otherwise undetectable microorganisms in cerebrospinal fluid.
Other tests
To identify the cause, doctors may also need to culture samples of blood and urine or to biopsy infected meninges or other tissues, which are identified using magnetic resonance imaging (MRI) or CT. Sometimes MRI or CT is done when the cause of symptoms is unclear.
Even after extensive testing, the cause often cannot be determined.
Prognosis for Subacute and Chronic Meningitis
The prognosis for people with subacute or chronic meningitis depends on
What is the cause is
In many cases, how strong the person's immune system is
Syphilis and Lyme disease usually resolve after treatment. Meningitis due to fungal or parasitic infections is harder to treat and more likely to recur, especially in people with HIV infection.
If meningitis is due to leukemia, lymphoma, or cancer, the prognosis is often poor. In such cases, meningitis can be fatal.
Treatment of Subacute and Chronic Meningitis
Treatment of the cause
Doctors focus on treating the cause. Depending on the cause, the following treatments are used:
For tuberculosis, syphilis, Lyme disease, or another bacterial infection: Antibiotics effective for the particular bacteria
For disorders that are not infections, such as sarcoidosis and Behçet syndrome: Corticosteroids or other drugs that suppress the immune system (immunosuppressants), sometimes taken for a long time
For spread of cancer to the meninges: A combination of radiation therapy directed at the head and/or chemotherapy, depending on the cancer
Chronic meningitis due to Cryptococcus neoformans






